Odisha Doctors' Strike Enters Crucial Phase: Why OMSA Wants Central-Style DACP, Pay Parity & KBK Exit Policy — And What a State-by-State Reality Check Reveals
Key Points
The Odisha government has called for formal talks on July 4 following three days of medical disruptions across peripheral public health centers.
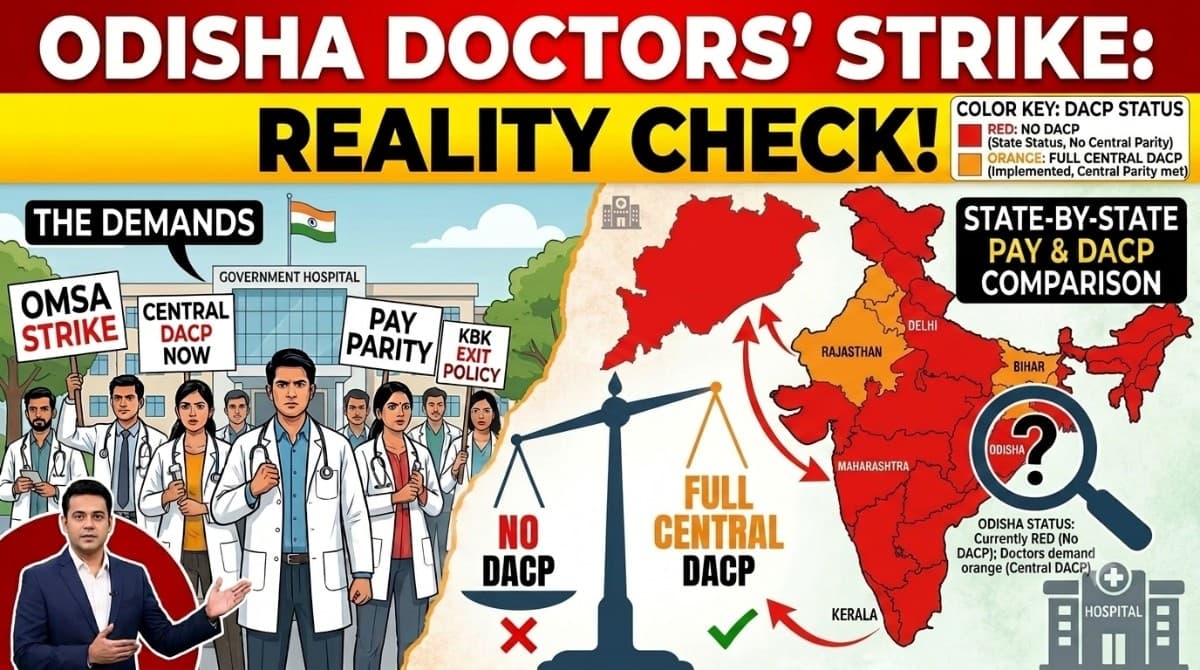
OMSA is demanding a transition from Odisha’s current 6-12-18-24 year promotional model to the automated 4-9-13-20 year Central Government DACP structure.
A state-by-state analysis reveals that only a few states like Delhi, Rajasthan, Punjab, Haryana, Bihar, and Jharkhand have implemented full central-parity DACP.
Bhubaneswar: After invoking the Odisha Essential Services (Maintenance) Act (ESMA), warning of salary deductions and disciplinary action against striking doctors, the Odisha government has finally opened the door for formal negotiations.
In a letter issued on Friday, the State Health Minister Mukesh Mahaling invited the Odisha Medical Services Association (OMSA) leadership for talks on July 4 at 11.30 am, while simultaneously appealing to the association to withdraw the indefinite strike and restore healthcare services across the state.
The invitation marks a significant shift in the government's approach after three days of disruption in public healthcare.
Ironically, the biggest flashpoint behind the agitation is Dynamic Assured Career Progression (DACP) – a framework first adopted by the previous Naveen Patnaik-led BJD government by replacing MACP with a modified DACP model, and subsequently continued by the present BJP government.
However, doctors under the OMSA banner argue that while Odisha calls its system DACP, it substantially differs from the Central Government's DACP, leaving them at a career and financial disadvantage.
The resulting deadlock has affected outpatient and inpatient services across PHCs, CHCs and several district hospitals, although emergency services and major medical colleges have continued functioning under pressure.
OMSA's Core Demands
The indefinite strike launched on July 1 (National Doctors' Day) revolves around a 10-point charter of demands that the association says has remained unresolved despite repeated assurances.
The principal demands include:
- Implementation of Central Government pattern DACP with promotions at 4, 9, 13 and 20 years instead of Odisha's present 6, 12, 18 and 24-year structure.
- Abolition of the Level-15 pay bottleneck and correction of pay anomalies affecting Odisha Medical and Health Service doctors.
- Transparent cadre restructuring and time-bound promotions.
- Amendment of the Odisha Medicare Act to make assaults on doctors non-bailable offences and deployment of 24×7 armed security in hospitals.
- Transparent transfer policy with a guaranteed exit after three years from KBK and difficult tribal postings.
- Regularisation of ad hoc doctors and reforms in administrative policies governing postings and promotions.
Demand No. 1: DACP – The Biggest Bone of Contention
The demand dominating the agitation is DACP.
Here lies the central misunderstanding.
Odisha already has a DACP scheme, introduced during the previous BJD government after replacing MACP. The BJP government has continued implementing the same policy.
However, OMSA is not demanding introduction of DACP per se.
Instead, doctors seek adoption of the Central Government DACP timeline.
Current Odisha Model
Financial upgradations after:
- 6 years
- 12 years
- 18 years
- 24 years
Central Government Model
Time-bound promotions after:
- 4 years
- 9 years
- 13 years
- 20 years
Doctors argue the additional waiting period delays promotions, pension benefits and lifetime earnings, making Odisha less attractive than Central Health Services and several states that have adopted the Central pattern.
Reality Check: How Many States Actually Follow Central DACP?
The national picture is far more complex than often projected.
States such as Delhi, Rajasthan, Punjab, Haryana, Bihar and Jharkhand have substantially adopted or mirrored the Central DACP structure.
However, Odisha is not alone in following a modified system.
Neighbouring states including:
- Andhra Pradesh
- West Bengal
- Chhattisgarh
continue to rely largely on state-specific ACP or customised promotion structures instead of the fully automated Central DACP model.
Thus, Odisha's framework is neither unique nor an outlier, although it is less generous than the Central model.
Why Can't Odisha Simply Adopt the Central DACP?
Legally and financially, the issue is more complicated.
Two important judicial precedents explain why.
📱 Get Argus News App
✨Supreme Court's Position
In Union of India vs K.P. Singh (2017), the Supreme Court observed that extending DACP has significant financial and structural implications. The Court held that such policy decisions require executive consideration and cannot be judicially imposed across cadres.
Allahabad High Court's Ruling
In Provincial Medical Service Officers Retired Welfare Association vs State of Uttar Pradesh (2025), the Allahabad High Court ruled that choosing between ACP and DACP is fundamentally a state policy decision.
The Court declined to direct Uttar Pradesh to adopt Rajasthan's or Delhi's DACP merely because they offered faster promotions.
This ruling effectively strengthens the argument that states retain discretion over career progression policies based on their financial capacity.
But There Is Another Judicial View
The Jharkhand High Court (2025) held that once a state adopts DACP, it cannot discriminate between similarly placed doctors within the same cadre.
The judgment dealt with parity within the state's own medical services rather than compelling adoption of the Central pattern.
Therefore, while courts recognise equality within cadres, they have generally refrained from directing states to replicate the Central DACP model.
Demand No. 2: Removal of Level-15 Bottleneck
OMSA argues that the existing Level-15 pay grade creates career stagnation for senior doctors.
Under the Central Health Service, movement into senior administrative grades is linked to structured career progression.
Doctors contend that Odisha's system leaves many officers waiting for vacancies before moving beyond Level-15, unlike other Group-A services where career progression is relatively smoother.
Whether the state can remove this bottleneck depends upon cadre restructuring, creation of additional posts and long-term fiscal commitments.
Demand No. 3: Three-Year Exit From KBK Areas
Doctors also seek a guaranteed exit after three years in difficult tribal and KBK postings.
Odisha's Position
The state has zoning guidelines, but shortages of specialists often result in doctors remaining far beyond intended tenures.
Comparison With Other States
Unlike Odisha, BJP-ruled states such as Uttar Pradesh and Madhya Pradesh primarily rely on compulsory rural service bonds for fresh graduates, backed by substantial penalties for non-compliance.
Some states like Rajasthan have introduced more transparent counselling-based transfer systems.
OMSA argues Odisha lacks an equally predictable exit mechanism once doctors complete difficult-area service.
Demand No. 4: Security of Doctors
Violence against doctors has emerged as another major issue.
OMSA demands:
- Non-bailable provisions against attackers. (which has been already implemented by an amendment to Orissa Medicare Service Persons and Medicare Service Institutions (Prevention of Violence and Damage to Property) Act, 2008)
- Permanent armed police deployment in hospitals.
The demand has gained momentum following incidents of attacks on doctors in Odisha, reinforcing concerns over workplace safety.
Demand No. 5: Pay Parity and Cadre Reforms
The association also seeks:
- Pay parity with other Group-A state services.
- Regularisation of ad hoc doctors.
- Transparent transfer policies.
- Faster promotions linked to service rather than vacancies.
These issues involve substantial administrative restructuring and carry long-term financial implications, making immediate implementation unlikely without detailed cabinet approval and finance department concurrence.
Bottom Line
The Odisha doctors' strike is not merely a dispute over salaries. It reflects a broader debate over how states should balance fiscal realities with retaining skilled medical professionals in public service.
On DACP, OMSA's demand for parity with the Central model finds support from doctors' career aspirations, but existing Supreme Court and High Court rulings also underscore that states retain considerable policy discretion over promotion structures and cannot be compelled to mirror the Centre solely through judicial intervention.
On rural postings, security and cadre reforms, several of OMSA's concerns echo challenges faced by doctors across India, though implementation models differ from state to state.
Politically, the episode also reveals a communication gap. OMSA had repeatedly warned of an escalation after months of representations, but the Health Department appeared to rely largely on verbal assurances until doctors finally switched off routine services.
Now, with
the Health Minister scheduled to hold direct talks with the association on July
4, both sides have an opportunity to convert confrontation into
negotiation. If the meeting yields a concrete roadmap rather than another round
of assurances, Odisha's healthcare system could begin returning to normal as
early as Saturday afternoon or Sunday.
Also Read: Nadda Launches SUMAN Roadmap 2030: 6 Odisha Districts Set for Special Maternal Healthcare Push Under 130-District National Mission | Special Story
Related Topics
Explore more stories